Showing posts with label CVDisease. Show all posts
Showing posts with label CVDisease. Show all posts
Thursday, November 15, 2012
Changes in CVD risk post-parathyroidectomy in PHPT
Effects of successful parathyroidectomy on metabolic cardiovascular risk factors in patients with severe primary hyperparathyroidism.
Ishay A, Herer P, Luboshitzky R.
[Endocrine Practice, 2011, Ishay, parathyroidectomy, DBP, CVD]
http://www.ncbi.nlm.nih.gov/pubmed/21324826
- study to evaluate effect of parathyroidectomy on metabolic abnormalities associated with CVD
- 34 Pt with HPT and 40 control patients with normal calcium assessed at baseline and 1 year later. HPT patients had parathyroidectomy
- significant decrease in DBP and insulin. significant increase in spine BMD
- no significant change in metabolic syndrome rate, insulin resistance, or likelihood of CVD risk
Thursday, November 20, 2008
Atorvostatin 80 mg vs 10 mg in stable CHD. Any real benefit?
This time the full TNT study is anlayzed at Paper Shredder.
See also a shredding of the subanalysis with regards to diabetics.
See also a shredding of the subanalysis with regards to diabetics.
Monday, November 17, 2008
Friday, November 14, 2008
Isn't it how you slice it?
From the PROactive study:
Lancet 2005 Oct 8;366(9493):1279-89




There is no significant reduction in the primary endpoint, but a reported reduction in the secondary endpoint which is a composite of all-cause mortality, non-fatal myocardial infarction and stroke.
But look at table 4: there is in fact no difference in each individual endpoint of death, non-fatal myocardial infarction (including silent MI), and stroke. Why is this?
A careful review of the article shows why. For the secondary endpoint they chose non-fatal myocardial infarction excluding silent MI. When this is thrown in you get figure 3 with an HR of 0.84 and CI of 0.72-0.98.
Does this really indicate anything significant about a reduction in macrovascular disease events when the data is manipulated in this way?
Lancet 2005 Oct 8;366(9493):1279-89




There is no significant reduction in the primary endpoint, but a reported reduction in the secondary endpoint which is a composite of all-cause mortality, non-fatal myocardial infarction and stroke.
But look at table 4: there is in fact no difference in each individual endpoint of death, non-fatal myocardial infarction (including silent MI), and stroke. Why is this?
A careful review of the article shows why. For the secondary endpoint they chose non-fatal myocardial infarction excluding silent MI. When this is thrown in you get figure 3 with an HR of 0.84 and CI of 0.72-0.98.
Does this really indicate anything significant about a reduction in macrovascular disease events when the data is manipulated in this way?

Tuesday, November 11, 2008
Legacy Effect not for Blood Pressure
Long-Term Follow-up after Tight Control of Blood Pressure in Type 2 Diabetes
Rury R. Holman, F.R.C.P., Sanjoy K. Paul, Ph.D., M. Angelyn Bethel, M.D., H. Andrew W. Neil, F.R.C.P., and David R. Matthews, F.R.C.P.
NEJM, Volume 359:1565-1576, october, 2008
ABSTRACT
Background
Post-trial monitoring of patients in the United Kingdom Prospective Diabetes Study (UKPDS) examined whether risk reductions for microvascular and macrovascular disease, achieved with the use of improved blood-pressure control during the trial, would be sustained.
Methods Among 5102 UKPDS patients with newly diagnosed type 2 diabetes mellitus, we randomly assigned, over a 4-year period beginning in 1987, 1148 patients with hypertension to tight or less-tight blood-pressure control regimens. The 884 patients who underwent post-trial monitoring were asked to attend annual UKPDS clinics for the first 5 years, but no attempt was made to maintain their previously assigned therapies. Annual questionnaires completed by patients and general practitioners were used to follow patients who were unable to attend the clinic in years 1 through 5, and questionnaires were used for all patients in years 6 to 10. Seven prespecified aggregate clinical end points were examined on an intention-to-treat basis, according to the previous randomization categories.
Results Differences in blood pressure between the two groups during the trial disappeared within 2 years after termination of the trial. Significant relative risk reductions found during the trial for any diabetes-related end point, diabetes-related death, microvascular disease, and stroke in the group receiving tight, as compared with less tight, blood-pressure control were not sustained during the post-trial follow-up. No risk reductions were seen during or after the trial for myocardial infarction or death from any cause, but a risk reduction for peripheral vascular disease associated with tight blood-pressure control became significant (P=0.02).
Conclusions The benefits of previously improved blood-pressure control were not sustained when between-group differences in blood pressure were lost. Early improvement in blood-pressure control in patients with both type 2 diabetes and hypertension was associated with a reduced risk of complications, but it appears that good blood-pressure control must be continued if the benefits are to be maintained.
Rury R. Holman, F.R.C.P., Sanjoy K. Paul, Ph.D., M. Angelyn Bethel, M.D., H. Andrew W. Neil, F.R.C.P., and David R. Matthews, F.R.C.P.
NEJM, Volume 359:1565-1576, october, 2008
ABSTRACT
Background
Post-trial monitoring of patients in the United Kingdom Prospective Diabetes Study (UKPDS) examined whether risk reductions for microvascular and macrovascular disease, achieved with the use of improved blood-pressure control during the trial, would be sustained.
Methods Among 5102 UKPDS patients with newly diagnosed type 2 diabetes mellitus, we randomly assigned, over a 4-year period beginning in 1987, 1148 patients with hypertension to tight or less-tight blood-pressure control regimens. The 884 patients who underwent post-trial monitoring were asked to attend annual UKPDS clinics for the first 5 years, but no attempt was made to maintain their previously assigned therapies. Annual questionnaires completed by patients and general practitioners were used to follow patients who were unable to attend the clinic in years 1 through 5, and questionnaires were used for all patients in years 6 to 10. Seven prespecified aggregate clinical end points were examined on an intention-to-treat basis, according to the previous randomization categories.
Results Differences in blood pressure between the two groups during the trial disappeared within 2 years after termination of the trial. Significant relative risk reductions found during the trial for any diabetes-related end point, diabetes-related death, microvascular disease, and stroke in the group receiving tight, as compared with less tight, blood-pressure control were not sustained during the post-trial follow-up. No risk reductions were seen during or after the trial for myocardial infarction or death from any cause, but a risk reduction for peripheral vascular disease associated with tight blood-pressure control became significant (P=0.02).
Conclusions The benefits of previously improved blood-pressure control were not sustained when between-group differences in blood pressure were lost. Early improvement in blood-pressure control in patients with both type 2 diabetes and hypertension was associated with a reduced risk of complications, but it appears that good blood-pressure control must be continued if the benefits are to be maintained.
UKPDS Follow-up NEJM
10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes.
Rury R. Holman, F.R.C.P. (click here for full article).
Methods: 5102 patients with newly diagnosed type 2 diabetes, 4209 were randomly assigned to receive either conventional therapy (dietary restriction) or intensive therapy (either sulfonylurea or insulin or, in overweight patients, metformin) for glucose control.

Results: Between-group differences in glycated hemoglobin levels were lost after the first year.

In the sulfonylurea–insulin group, relative reductions in risk persisted at 10 years for any diabetes-related end point (9%, P=0.04) and microvascular disease (24%, P=0.001), and risk reductions for myocardial infarction (15%, P=0.01) and death from any cause (13%, P=0.007) emerged over time, as more events occurred.


In the metformin group, significant risk reductions persisted for any diabetes-related end point (21%, P=0.01), myocardial infarction (33%, P=0.005), and death from any cause (27%, P=0.002).

Rury R. Holman, F.R.C.P. (click here for full article).
Methods: 5102 patients with newly diagnosed type 2 diabetes, 4209 were randomly assigned to receive either conventional therapy (dietary restriction) or intensive therapy (either sulfonylurea or insulin or, in overweight patients, metformin) for glucose control.

Results: Between-group differences in glycated hemoglobin levels were lost after the first year.

In the sulfonylurea–insulin group, relative reductions in risk persisted at 10 years for any diabetes-related end point (9%, P=0.04) and microvascular disease (24%, P=0.001), and risk reductions for myocardial infarction (15%, P=0.01) and death from any cause (13%, P=0.007) emerged over time, as more events occurred.

In the metformin group, significant risk reductions persisted for any diabetes-related end point (21%, P=0.01), myocardial infarction (33%, P=0.005), and death from any cause (27%, P=0.002).

Jupiter Study
Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein
Paul M Ridker, M.D. et al (click here for full article)
Methods: randomly assigned 17,802 healthy men and women with low-density lipoprotein (LDL) cholesterol levels of less than 130 mg per deciliter (3.4 mmol per liter) and high-sensitivity C-reactive protein levels of 2.0 mg per liter or higher to rosuvastatin, 20 mg daily, or placebo.
Paul M Ridker, M.D. et al (click here for full article)
Methods: randomly assigned 17,802 healthy men and women with low-density lipoprotein (LDL) cholesterol levels of less than 130 mg per deciliter (3.4 mmol per liter) and high-sensitivity C-reactive protein levels of 2.0 mg per liter or higher to rosuvastatin, 20 mg daily, or placebo.
Results: Rosuvastatin reduced LDL cholesterol levels by 50% and high-sensitivity C-reactive protein levels by 37%. The rates of the primary end point were 0.77 and 1.36 per 100 person-years of follow-up in the rosuvastatin and placebo groups, respectively (hazard ratio for rosuvastatin, 0.56; 95% confidence interval [CI], 0.46 to 0.69; P<0.00001)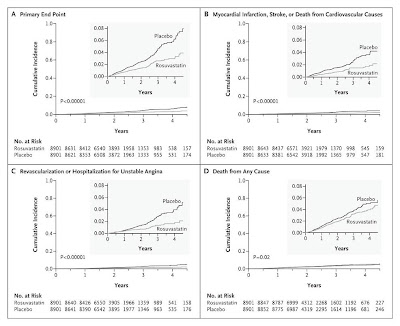
Figure 1: endpoint data
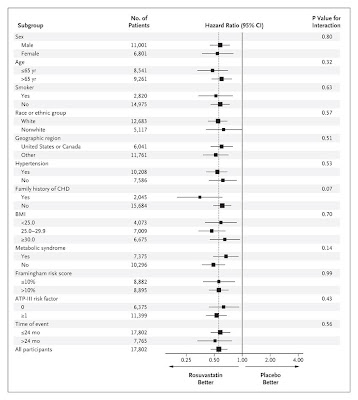
Figure 2: hazard ratio

Figure 1: endpoint data

Figure 2: hazard ratio
Subscribe to:
Posts (Atom)